Flu Vaccine Screening Questionnaire
Flu Vaccine Screening Questionnaire. Do you have a serious allergy to eggs? Injectable influenza vaccination screening questionnaire for adult patients as well as parents of children to be vaccinated:
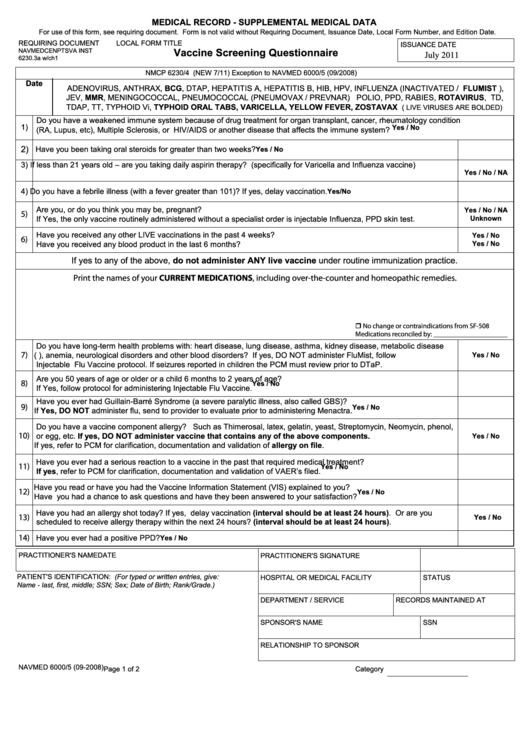
Yes no don’t know 1. If you answer “yes” to any question, it does not necessarily mean you (or your child) should not be vaccinated. Wegmans pharmacy informed consent/screening questionnaire to receive inactivated injectable influenza vaccine (ny) name:
This Checklist Helps Decide About Vaccinating You Or Your Child Today.
Always screen patients for contraindications and precautions before a vaccine is administered, even if the same vaccine was administered previously. Has a disease that lowers immunity (eg leukaemia, cancer, hiv) or is having treatment that lowers immunity (eg oral steroid medicines such as cortisone and prednisone. The following questions will help us determine if there is any reason we should not give you or your child inactivated injectable influenza vaccination today.
Wegmans Pharmacy Informed Consent/Screening Questionnaire To Receive Inactivated Injectable Influenza Vaccine (Ny) Name:
Please fill in the following information for your doctor/nurse. For adult patients as well as parents of children to be vaccinated: People who have experienced a severe or life threatening allergic reaction (e.g., anaphylaxis) to a prior dose of any influenza vaccine.;
Signature Of Person Receiving Vaccine Or Parent/Guardian O Influenza Virus Vaccine, Quadrivalent (Iiv4),.5 Ml, Im ( 6 Months And Older) O Influenza Virus Vaccine (Iiv), Enhanced Immunogenicity (High Dose).5Ml (65 And Over) O Influenza Virus Vaccine, Quadrivalent (Riv4), Derived From Recombinant Dna,.5 Ml (Egg Free) (18 Years And Over)
_____ screening questionnaire for vaccination the following questions help us determine which vaccines you may be given today. _____ primary care or other physician: October 5, 2020 section 1:
Information For Health Professionals About The Screening Questionnaire For Inactivated Injectable Influenza Vaccination Are You Interested In Knowing Why We Included A Certain Question On The Screening Questionnaire?
Screening checklist for contraindications to live attenuated intranasal influenza vaccination keywords: If a question is not clear, please ask your nurse to explain it. Influenza injectable place rx label here o o pneumococcal hepatitis b hpv o varicella o ipv:
Infants Younger Than 6 Months Of Age.
If you answer “yes” to any question, it does not necessarily mean you (or your child) should not be vaccinated. If you answered yes to any of the questions a screener will help you decide which vaccine is right for you. The following questions will help us determine if there is any reason we should not give you or your child injectable influenza vaccination today.
{kind=link}
Post a Comment for "Flu Vaccine Screening Questionnaire"